BME 256 - Feasibility of an Electrical Impedance Stethoscope
Abstract
Background
Continuous patient monitoring has great significance in healthcare, as constantly assessing vitals is crucial for accurate prognosis during disease progression and for providing an updated course of treatment for said prognosis. Heart rate, respiratory rate, and blood pressure are all key values that exhibit patient condition and are traditionally measured via separate devices. The purpose of this study is to assess the feasibility of a new medical device--the electrical impedance stethoscope (EIS)--for its capacity to integrate all necessary vital readings into a singular non-invasive sensor.
Methods
The EIS concept involves measuring impedance between flexible patch electrodes placed on the anterior chest over the heart and left posterior chest wall. This study focuses on preliminary exploration of the device and primarily utilizes algebraic expressions, standard integration, and computational modeling techniques to simulate impedance changes across the cardiac and respiratory cycles. Equations are derived to calculate time-varying resistances of the heart and lung models, incorporating factors such as blood volume and lung expansion in their respective systems. Classic digital signaling processes are then performed on patient vital data, including low-pass filtering and peak detection to create the most accurate signal. A final validation is done by comparing normal filtered impedance data to that of someone undergoing cardiac or hemorrhagic shock.
Results
Simulation studies demonstrate time-varying impedance signals representative of cardiac and respiratory activity. Incorporating shunt resistance to account for current paths through the body wall and mediastinum significantly reduces total chest impedance, aligning with physiological expectations. Further processing demonstrates the filtering of two distinct waveforms that represent respiratory and cardiac function as separate readings. The simulations were also run for hemorrhagic and cardiogenic shock situations.
Conclusion
The simulations suggest the potential of the EIS as a viable method for continuous vital sign monitoring. By leveraging computational modeling and digital signal processing techniques, it’s possible to extract cardiac and respiratory waveforms from impedance signals, paving the way for further investigation and development of this integrated monitoring system. Future work will focus on refining signal processing algorithms and conducting real-time testing to validate the concept's clinical utility.
Time-Varying Chest Resistance Model
The initial model was based on sinusoidal functions of the heart and lungs. The high frequency wave represents the impedance due to the heart, while the underlying wave represents the lungs.
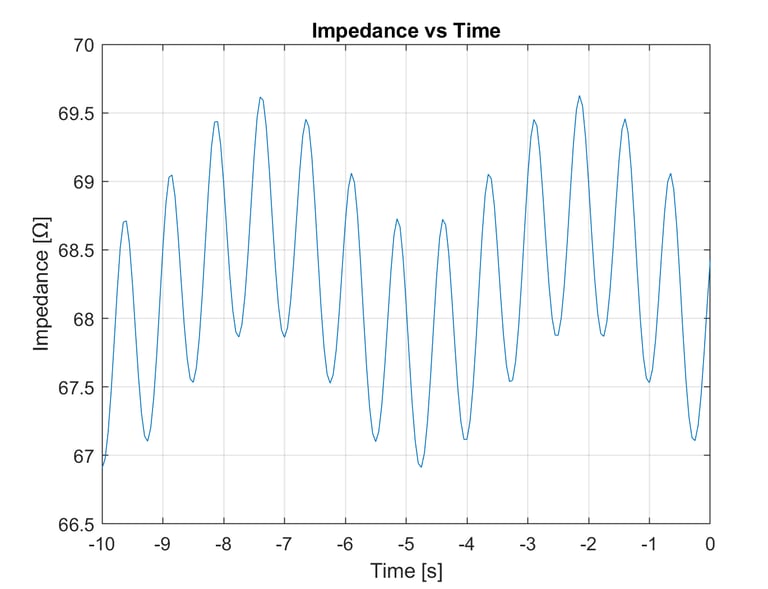
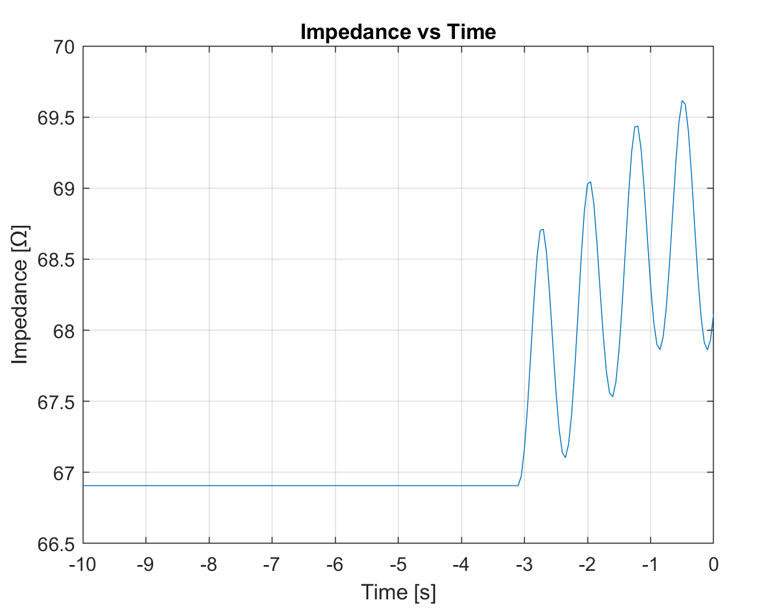
Real-Time Scrolling Display
A realistic monitoring system would require constant data recording and a moving display. Using the same model above, we created a real-time scrolling display from current time to 10 seconds in the past.
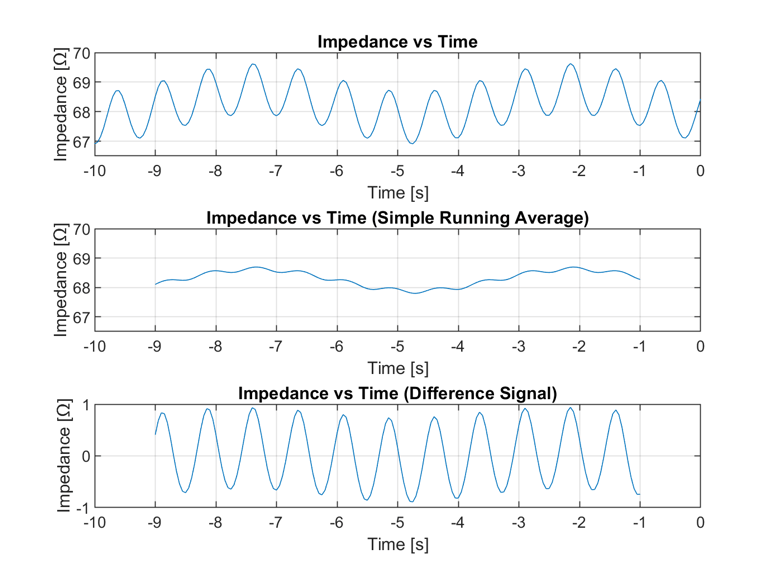
Simple Running Average
Used a simple funning average to extract the lung and cardiac signals. The window for the average to be taken was 2 seconds, so the first and last second of input data cannot have a valid average.
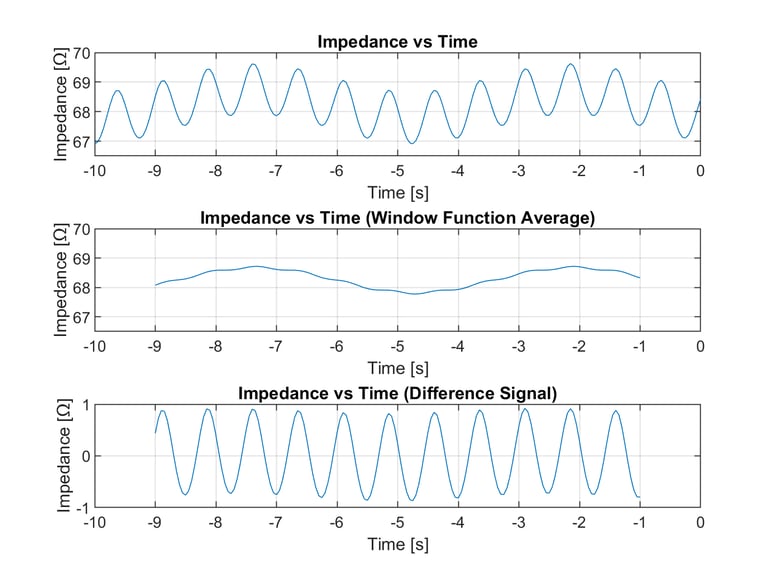
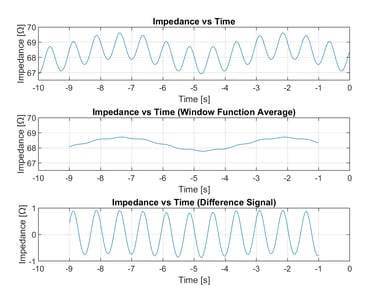
Windowing Function Running Average
A slightly more complex averaging function was used. This windowing function used 2 seconds windows and weighted the values according to their location relative to the center point. Therefore, data points closer to the center would carry a greater weight in determining the average value for that point.
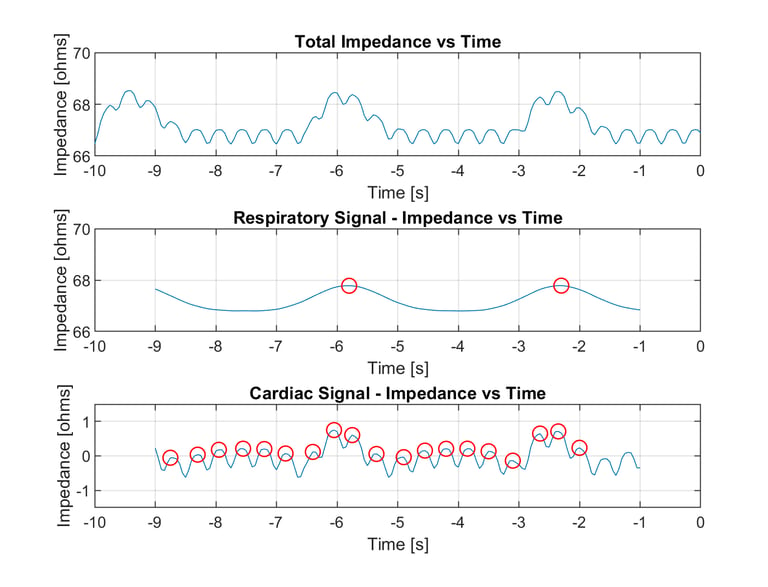
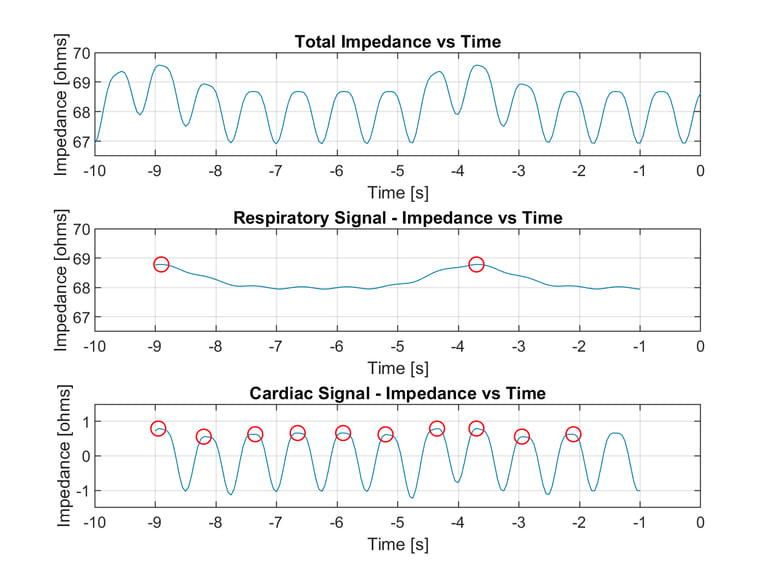
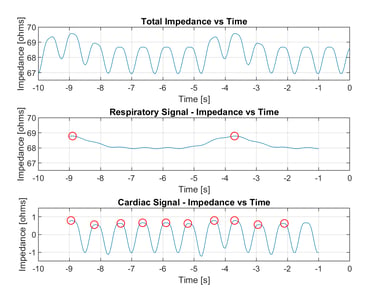
Peak Detection
A peak detection algorithm was implemented to determine the respiratory rate and heart rate.
Simulated Cardiogenic Shock
The model we created can be used to simulate failure scenarios related to the circulatory system. This includes cardiogenic shock as one example.